ADHD, ASD and AuDHD ASSESSMENT UPDATE:
We’re currently at capacity for our ADHD, AuDHD and ASD assessments right now but will resume soon. Please check here for regular updates.
All other services still available
Get in touch
GP referrals please follow this link
Physical Address
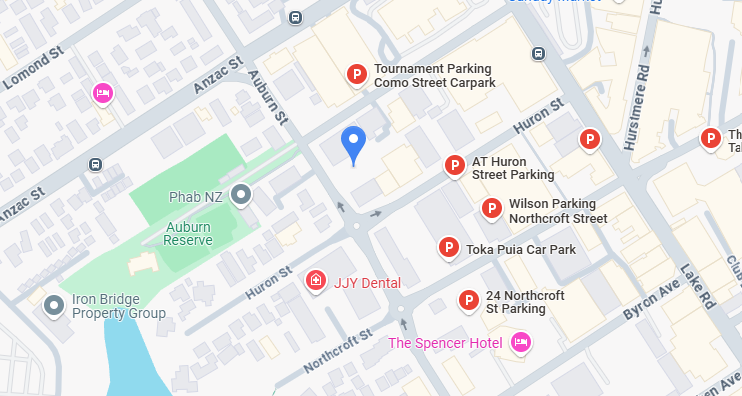
Takapuna Clinic
Level 1, 5 Auburn St
Takapuna
Auckland
Warkworth Clinic
Level 1, Kowhai Medical
4 Warkworth Street
Warkworth
-
For all other enquiries, please contact us at
phone: (09) 320 3086
- email: admin@psyched.org.nz
-
email: accounts@psyched.org.nz
SELF REFFERAL FORM
"*" indicates required fields